OUTDATED
This version is outdated. Please see https://doi.org/10.47326/ocsat.2021.02.17.2.0 for the latest version of this Science Brief.
Key Message
This Science Brief provides information for health care professionals about Vaccine-Induced Prothrombotic Immune Thrombocytopenia (VIPIT), a rare adverse event following the AstraZeneca COVID-19 vaccine.
This brief describes the pathophysiology, presentation, diagnostic work-up and treatment of VIPIT. Figure 1 presents a decision tree for diagnosing and ruling out VIPIT.
Lay Summary
What do we know so far?
The United Kingdom, European Union, and Scandinavian countries have reported that the AstraZeneca COVID-19 vaccine appears to be associated with rare cases of serious blood clots, including blood clots in the brain. These blood clots have two important features: they occur 4 to 20 days after vaccination, and they are associated with low platelets (tiny blood cells that help form blood clots to stop bleeding). Doctors are calling this “vaccine-induced prothrombotic immune thrombocytopenia” (VIPIT). VIPIT seems to be rare, occurring in anywhere from 1 in every 125,000 to 1 in 1 million people.
Health Canada has stated that the AstraZeneca COVID-19 vaccine continues to be safe and effective at protecting Canadians against COVID-19 and encourages people to get immunized with any of the COVID-19 vaccines that are authorized in Canada.
Are certain people more likely to get VIPIT?
VIPIT is very rare. At this time, we do not know if certain patients are more likely to get VIPIT. So far, most of the cases from Europe have occurred in women under age 55 – but many of these countries used more of their initial AstraZeneca vaccine supply in women under age 55. We do not believe that VIPIT is more common in people who have had blood clots before, people with a family history of blood clots, people with a low platelets, or pregnant women, because VIPIT does not develop through the same process as usual types of bleeding or clotting problems.
What should you look out for if you received the AstraZeneca COVID-19 vaccine?
You should speak to a health care professional if you have unusual or severe symptoms after any COVID-19 vaccine. If you experience the following symptoms between 4 and 20 days after vaccination, it might indicate that you have VIPIT: a severe headache that does not go away; a seizure; difficulty moving part of your body; new blurry vision that does not go away; difficulty speaking; shortness of breath; chest pain; severe abdominal pain; new severe swelling, pain, or colour change of an arm or a leg. These symptoms can also be a sign of other serious conditions and should be assessed in an emergency department.
What should you do if you have concerning symptoms after the AstraZeneca COVID-19 vaccine?
If your symptoms are not severe, you can see (virtually or in-person) your primary care professional. If you have severe symptoms, you should go to the nearest emergency department immediately. You should tell the health care providers who see you that you received the AstraZeneca COVID-19 vaccine and give them the date you got vaccinated. If the healthcare professional who assesses you is concerned, you may have scans and additional bloodwork collected.
Do healthcare professionals know how to diagnose and treat VIPIT?
Yes. Health care professionals and scientists in Ontario have been working with experts in Canada, and around the world, to better understand VIPIT. The Ontario COVID-19 Science Advisory Table has summarized what we know about VIPIT right now and has published guides for healthcare professionals outside and inside the hospital, to help them diagnose and treat VIPIT.
Why is Ontario still using the AstraZeneca COVID-19 vaccine?
Health Canada reviewed the AstraZeneca COVID-19 Vaccine, as well as a similar vaccine called COVISHIELD. They have stated that the benefits in protecting Canadians from COVID-19 continue to outweigh the risks and encourage Canadians to get immunized with any of the COVID-19 vaccines that are authorized in Canada when they are eligible. Keep in mind that COVID-19 has killed over 15,000 Canadians so far, that about 1 in 100 Canadians who get COVID-19 end up needing intensive care, and that 1 in 5 Canadians who are hospitalized with COVID-19 develop blood clots. Currently Canada is experiencing a third wave of COVID-19. VIPIT is very rare, while the AstraZeneca vaccine has proven effective at reducing severe illness from COVID-19. Health care professionals, scientists, and government agencies in Ontario – and around the world – will continue to monitor the safety of this and all vaccines.
Could other COVID-19 vaccines available in Ontario cause VIPIT?
There have been no confirmed cases of VIPIT with any other COVID-19 vaccine.
Full Text
Background
The AstraZeneca COVID-19 vaccine appears to be associated with autoimmune thrombosis that mimics heparin-induced thrombocytopenia.
The United Kingdom, European Union, and Scandinavian countries have reported rare cases of cerebral sinus vein thrombosis (CSVT) and thrombocytopenia in patients who received the AstraZeneca COVID-19 vaccine. The majority of affected patients thus far are women under the age of 55 years, and CSVT seems to occur 4 to 20 days after vaccination. The Paul Ehrlich Institute has demonstrated that affected individuals in Germany have antibodies that induce massive platelet activation, reducing the platelet count and causing thrombosis.1This phenomenon mimics heparin-induced thrombocytopenia (HIT) yet it does not require heparin as a trigger. It has been named vaccine-induced prothrombotic immune thrombocytopenia (VIPIT).
Questions
How frequent is VIPIT?
Are certain patients predisposed to VIPIT?
When should I suspect my patient has VIPIT?
How do I diagnose VIPIT? How do I rule it out?
How do I treat VIPIT?
How do I treat VIPIT with life threatening blood clots?
Is VIPIT a reportable event?
Can patients who develop VIPIT safely receive a second dose of AstraZeneca’s COVID-19 vaccine? Can they receive another COVID-19 vaccine?
Findings
How frequent is VIPIT?
To date, millions of AstraZeneca COVID-19 vaccine doses have been administered worldwide, with suspected cases of VIPIT occurring in only a small fraction of vaccinated individuals. However, there is growing evidence of a causal link with the vaccine. The incidence of VIPIT appears to be between 1 in 125,000 and 1 in 1 million.2
There is no evidence that the AstraZeneca COVID-19 vaccine increases the overall risk of thrombosis (e.g., deep vein thromboses, pulmonary emboli, myocardial infarction, stroke) beyond what is seen in the general population despite the observed increases in CSVT, as the risk of CSVT is orders of magnitude lower than the risk of other thromboses. The AstraZeneca COVID-19 vaccine is highly effective in preventing COVID-19, which also carries a high risk of thrombosis; 1 in 5 patients hospitalized with COVID-19 develops venous thrombosis.3 For this reason, Health Canada, the United Kingdom Medicines and Healthcare Products Regulatory Agency, and the European Medicines Agency have recommended to continue administering the AstraZeneca COVID-19 vaccine, and have all made clear statements about their assessment of risks and benefits in the setting of the COVID-19 pandemic.2,4,5 Physicians, scientists, and regulatory agencies worldwide will continue to carefully monitor the safety of the AstraZeneca vaccine and of COVISHIELD, the version of the AstraZeneca COVID-19 vaccine currently available in Canada.
Are certain patients predisposed to VIPIT?
At this time, it is not clear if certain patients are predisposed to VIPIT. The cases to date are predominantly in younger women, however these individuals may have been overrepresented in the vaccinated population in European Union countries.2 Further information from jurisdictions like the United Kingdom that prioritized older adults for early vaccination is pending. Since VIPIT is immune-mediated, an individual with a thrombophilia, a family history of blood clots, or a personal history of arterial or venous clots would likely not be at increased of VIPIT. Accordingly, there are no new contraindications to receiving the AstraZeneca vaccine.
When should I suspect my patient has VIPIT?
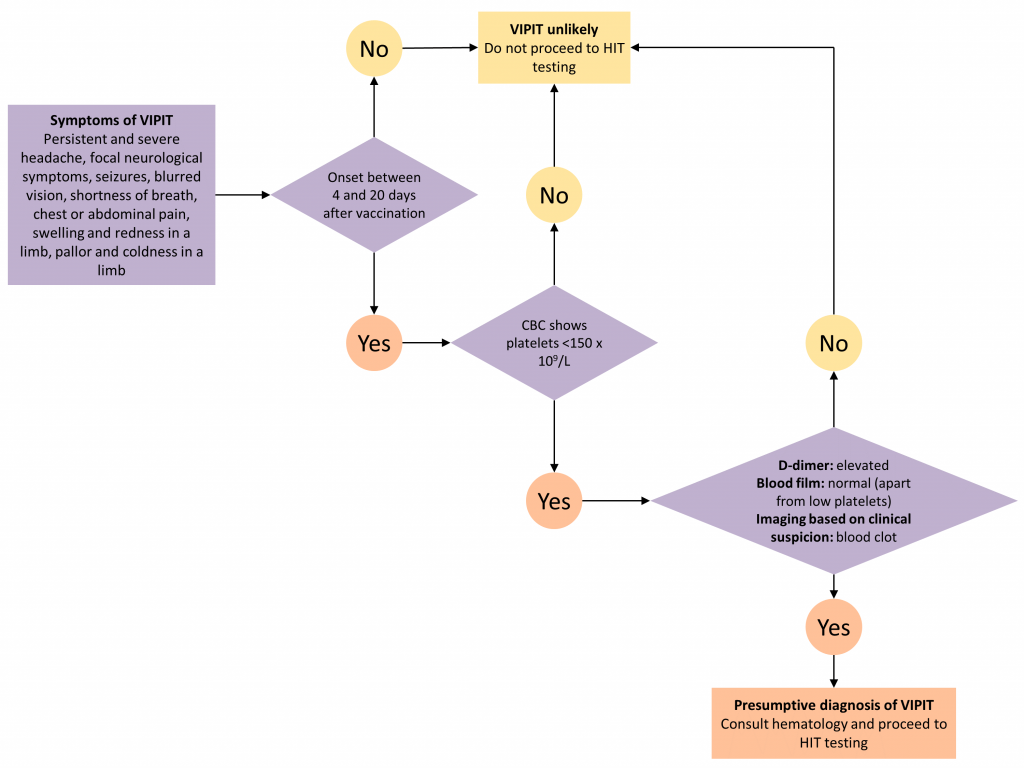
Patients with VIPIT may present with CSVT, or with other arterial or venous clots. Any patient with unusual symptoms following vaccination should be assessed by a health care provider. Some symptoms make it more likely that a patient has VIPIT: persistent and severe headache; focal neurological symptoms (including blurred vision); shortness of breath; abdominal or chest pain; swelling and redness in a limb; or pallor and coldness in a limb. VIPIT seems to occur between 4 to 20 days post-vaccination. Symptoms in this time frame should raise the clinical suspicion of VIPIT.
How do I diagnose VIPIT? How do I rule it out?
Patients with severe symptoms should urgently seek care at their nearest emergency department. Patients with non-severe symptoms may have initial investigations done in the primary care or outpatient setting.
Clinicians should ask patients about their COVID-19 vaccine history and should draw a complete blood count (CBC). VIPIT is unlikely if symptoms of blood clotting fall outside of the 4 to 20 day time frame OR if the platelet count is ≥ 150 x 109/L.6 VIPIT is more likely if symptoms of blood clotting fall within the 4 to 20 day time frame AND the platelet count is < 150 x 109/L, and such patients should be evaluated at their nearest emergency department for suspected VIPIT. This will expedite further diagnostic workup, treatment, and urgent hematology consultation.
Patients with suspected VIPIT should go on to have blood work drawn including a D-dimer level and a blood film. When there is strong clinical suspicion of VIPIT, patients should also have diagnostic imaging to investigate for blood clots (including appropriate imaging to rule out CSVT, if the patient presents with a persistent and severe headache). It is not known whether VIPIT, like HIT, is associated with arterial thromboses, but arterial clots should be considered if patients have consistent symptoms. An elevated D-dimer, a normal blood film (apart from thrombocytopenia), and confirmation of a blood clot on diagnostic imaging makes the diagnosis of VIPIT presumptive.
The confirmatory diagnosis of VIPIT is made by testing for HIT. This testing should be done even if the patient has had no previous exposure to heparin. HIT testing involves two steps: identification of antibodies against the complex of platelet factor 4 and heparin; and confirmatory functional testing of the antibodies’ ability to activate platelets.7 The HIT antibody test appears very sensitive to VIPIT; if it is positive, VIPIT is confirmed, and if it is negative, VIPIT is unlikely.1
A number of large hospital laboratories test for HIT antibodies, but only one lab in Canada performs confirmatory functional testing (the McMaster University Platelet Immunology Laboratory). Therefore, presumptive VIPIT should prompt an urgent hematology consultation (in person, virtually, or by phone) to arrange testing and start safe empiric treatment of blood clots (see below).
How do I treat VIPIT?
Patients with presumptive and confirmed VIPIT should be treated similarly to HIT. The Box presents the treatment principles for patients with presumptive and confirmed VIPIT. Until VIPIT has been ruled out, anticoagulation with heparin (unfractionated heparin and low molecular weight heparins) should be avoided. Platelet transfusions should not be given.
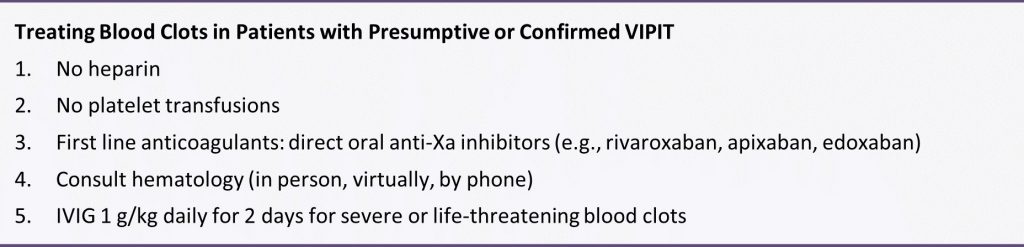
Alternative anticoagulants that are safe to use in HIT, and likely safe to use in VIPIT, include direct thrombin inhibitors and anti-Xa inhibitors. Most clinicians in Ontario will be comfortable using direct oral anti-Xa inhibitors (e.g., rivaroxaban, apixaban, edoxaban) empirically while awaiting further advice from a hematologist; these agents are used in the treatment of HIT. The dose of direct oral anti-Xa inhibitor is identical to the dose used to treat uncomplicated deep vein thromboses. If the patient has severe renal impairment that makes direct oral anticoagulants unsafe, advice from a hematologist should be sought to guide use of parenteral anticoagulants that are safe to use in HIT.
How do I treat VIPIT with life threatening blood clots?
In patients with confirmed VIPIT and severe or life-threatening blood clots (e.g., CSVT, splanchnic vein thrombosis), it is important to dampen the prothrombotic response with intravenous immunoglobulin (IVIG). Administration of high dose IVIG (1 g/kg of body weight daily for two days) is appropriate and can be guided by the consulting hematologist.
Is VIPIT a reportable event?
All suspected adverse events following immunization (AEFI), including thrombosis, and both presumptive and confirmed VIPIT, should be reported using the provincial AEFI form and sent to the local Public Health Unit. More information on how to report AEFIs can be found on the Public Health Ontario website. Ontario conducts vaccine surveillance safety in collaboration with the Public Health Agency of Canada, and prompt reporting is essential to learn more about this rare but serious thrombotic phenomenon.
Can patients who develop VIPIT safely receive a second dose of AstraZeneca’s COVID-19 vaccine? Can they receive another COVID-19 vaccine?
At this time, we do not know how subsequent doses of COVID-19 vaccines should be managed in individuals who develop VIPIT following their first dose. These cases require consultation with a hematologist. We know that individuals with non-vaccine associated HIT can be safely re-exposed to heparin, under very controlled conditions, but this requires the advice and close monitoring of a hematologist. This is an area of active study. There have been no confirmed cases of VIPIT with any other COVID-19 vaccine. Therefore, a second dose of another COVID-19 vaccine may be safe.
Interpretation
VIPIT is a rare adverse event following the AstraZeneca COVID-19 vaccine. This brief describes the pathophysiology, presentation, diagnostic work-up and treatment of VIPIT, including a decision tree for diagnosing and ruling out VIPIT.
References
1. Updated GTH statement on vaccination with the AstraZeneca COVID-19 vaccine, as of March 22, 2021. Published March 18, 2021. Accessed March 24, 2021. https://gth-online.org/wp-content/uploads/2021/03/GTH_Stellungnahme_AstraZeneca_3_24_2021.pdf
2. PINHO AC. COVID-19 Vaccine AstraZeneca: benefits still outweigh the risks despite possible link to rare blood clots with low platelets. European Medicines Agency. Published March 18, 2021. Accessed March 24, 2021. https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazeneca-benefits-still-outweigh-risks-despite-possible-link-rare-blood-clots
3. Malas MB, Naazie IN, Elsayed N, Mathlouthi A, Marmor R, Clary B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: A systematic review and meta-analysis. EClinicalMedicine. 2020;29:100639. https://doi.org/10.1016/j.eclinm.2020.100639
4. Health Canada confirms that the benefits of the AstraZeneca COVID-19 vaccine continue to outweigh the risks for use in Canada. Health Canada. Published March 18, 2021. Accessed March 24, 2021. https://www.canada.ca/en/health-canada/news/2021/03/health-canada-confirms-that-the-benefits-of-the-astrazeneca-covid-19-vaccine-continue-to-outweigh-the-risks-for-use-in-canada.html
5. UK regulator confirms that people should continue to receive the COVID-19 vaccine AstraZeneca. GOV.UK. Accessed March 24, 2021. https://www.gov.uk/government/news/uk-regulator-confirms-that-people-should-continue-to-receive-the-covid-19-vaccine-astrazeneca
6. Warkentin TE. Heparin-induced thrombocytopenia: pathogenesis and management. Br J Haematol. 2003;121(4):535-555. https://doi.org/10.1046/j.1365-2141.2003.04334.x
7. Greinacher A, Selleng K, Warkentin TE. Autoimmune heparin-induced thrombocytopenia. J Thromb Haemost. 2017;15(11):2099-2114. https://doi.org/10.1111/jth.13813
Document Information & Citation
Author Contributions: MP, PJ and AMM conceived the Science Brief. MP wrote the first draft of the Science Brief. All authors contributed to the conception of the Science Brief, revised it critically for important intellectual content and approved the final version.
Citation: Pai M, Grill A, Ivers N, et al. Vaccine induced prothrombotic immune thrombocytopenia VIPIT following AstraZeneca COVID-19 vaccination. Science Briefs of the Ontario COVID-19 Science Advisory Table. 2021;1(17). https://doi.org/10.47326/ocsat.2021.02.17.1.0
Author Affiliations: The affiliations of the members of the Ontario COVID-19 Science Advisory Table can be found at https://covid19-sciencetable.ca/.
Declarations of Interest: The declarations of interest of the members of the Ontario COVID-19 Science Advisory Table, its Working Groups, or its partners can be found at https://covid19-sciencetable.ca/.
Copyright: 2021 Ontario COVID-19 Science Advisory Table. This is an open access document distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided that the original work is properly cited.
The views and findings expressed in this Science Brief are those of the authors and do not necessarily reflect the views of all of the members of the Ontario COVID-19 Science Advisory Table, its Working Groups, or its partners.